

Management of curved canal
Curved canals is cindered one of the hardest treatment facing the dentist, because of high chance of file separation or creating a ledge canal, in the past the management was with manual files, the dentist pre pent the manual files and starts negotiating the curve canal starting from k file 8 till 25 or 30, this process takes long time and high effort from the patient and the dentist, and some times in slightly or moderate curved canal the management with high flexible rotary files is so far acceptable, but risky.
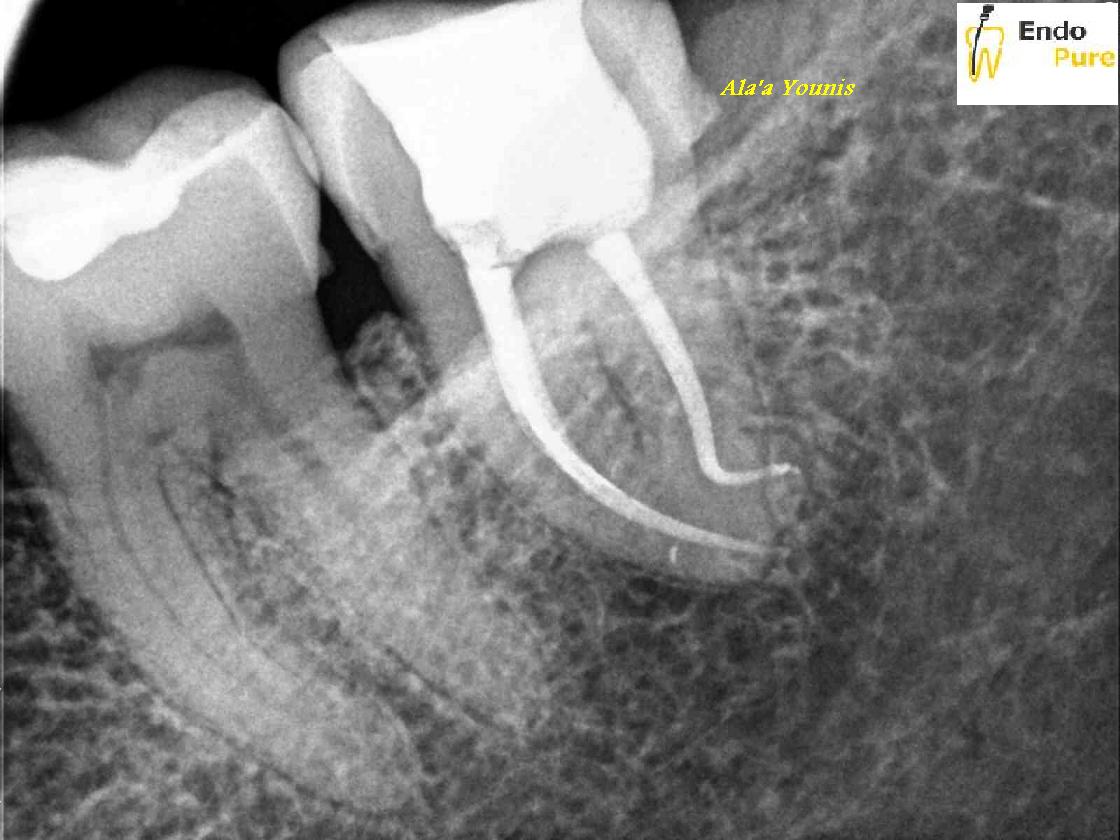
After the invention of controlled memory Ni Ti files, management of curved canals become more easy and safe, now you just flare the coronal third and scout with k10 till it become loose and some times till k15..then shape the canal according to the system you have. Controlled memory files decrease the chance of file separation in curved canals because of its high flexibility , also its decrease the time of the treatment as you don’t need for too much manual filings of the curve as before. In this case this ninety degree curve was treated with controlled memory files.
Most of the time the master apical file for the curve canal is 25 or 30 not more, as if you increase the size you may end with mishaps.
Obturation of curved canal usually is challenge, usually the master apical cone should be pre curved and place inside the canal and the dentist should check the tug back to provide good apical seal, and in some cases specially the double curved canals when the dentist use vertical compaction technique if the plugger of the heat pen not reaching 5 to 7 mm short than the apex , the dentist must shift to carrier based guttapercha (thermal) to obtain three dimensional obturation of the canal.